
HORMONES & AGING: What Changes, Why It Matters, and How to Optimize 𐂁
Hormones are chemical messengers. They help regulate energy, metabolism, mood, fertility, body composition, sleep, brain function, skin, hair, libido, and bone health. They are present in both women and men, just in different amounts and patterns. When hormones shift too far up, too far down, or become out of balance with one another, symptoms often show up long before a diagnosis does.
For many women, the conversation becomes most obvious in perimenopause and menopause, when estrogen and progesterone begin to fluctuate and eventually decline. But hormone issues are not just a menopause topic. Men can have hormone problems too, especially with testosterone, insulin, thyroid, and stress hormones. And in both sexes, symptoms can overlap with sleep issues, blood sugar problems, thyroid dysfunction, inflammation, medication effects, and lifestyle stress.
Hormones are not isolated. They work like an orchestra. If one section is off, the whole system can sound off. Low estrogen can affect sleep, skin, vaginal tissue, and bones. Low progesterone can affect sleep, cycle regularity, and mood. Testosterone affects libido, muscle, motivation, and body composition in both men and women. Thyroid can mimic menopause. Insulin can drive weight gain and inflammation. Cortisol can leave someone wired, tired, and struggling to recover.
That framing usually helps clients understand why a thorough lab review matters instead of chasing one symptom at a time.THE BIG PICTURE
Hormones are your body’s communication system.
They regulate:
Energy
Sleep
Mood
Weight & metabolism
Libido
Muscle & bone
Skin & hair
As we age, hormone production naturally declines.
But symptoms are not just “normal aging”—they are signals.
WHAT HAPPENS AS WE AGE
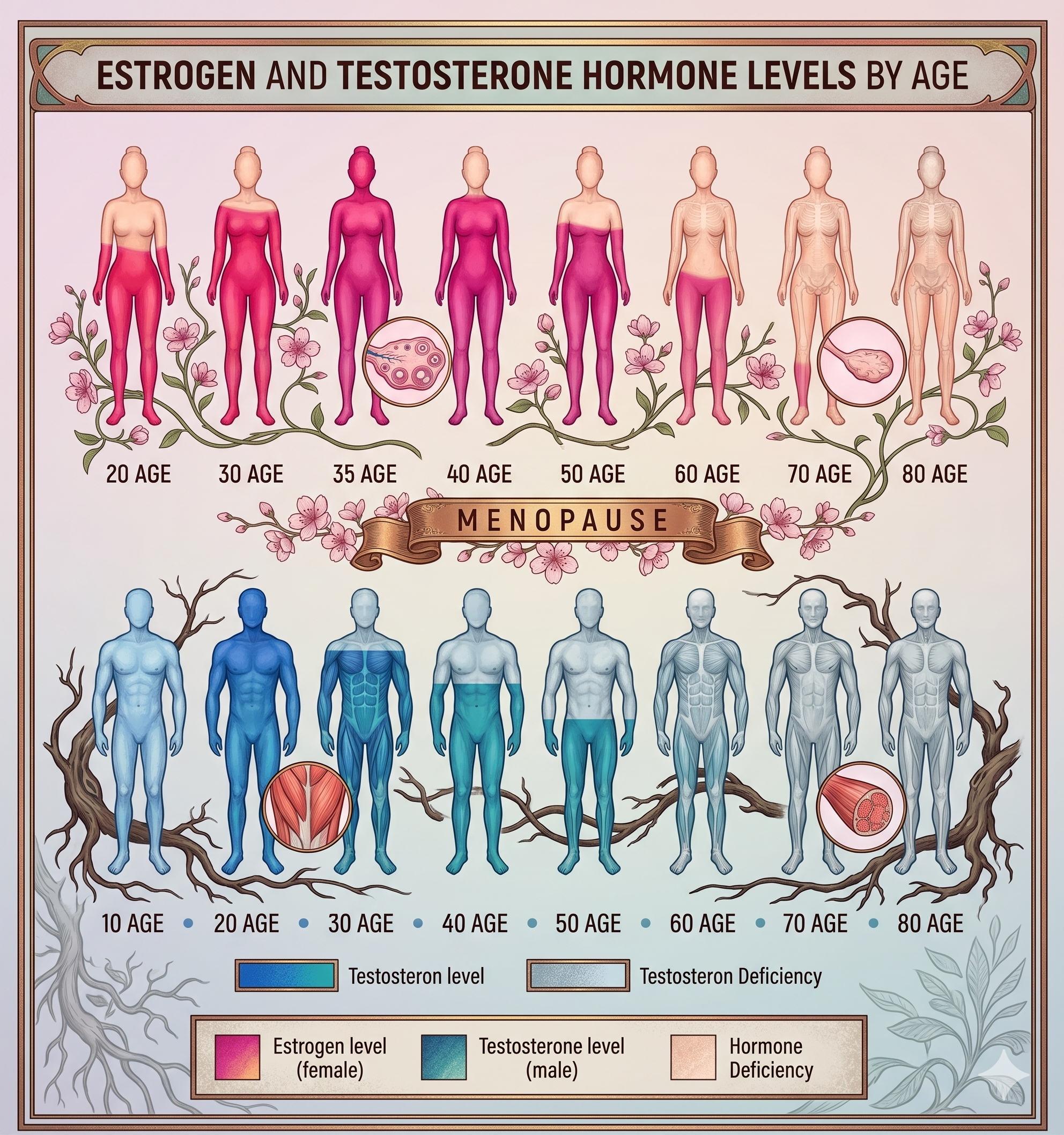
WOMEN: PERIMENOPAUSE → MENOPAUSE
Perimenopause (late 30s–40s)
Perimenopause is the transition leading up to menopause. During this time, estrogen can swing up and down, ovulation may become less predictable, and progesterone often becomes less steady because it depends on ovulation. This is why women in their late 30s and 40s may report irregular periods, poor sleep, anxiety, mood shifts, heavier cycles, breast tenderness, or feeling “off” even before periods stop.
Progesterone declines first
Estrogen fluctuates (up and down)
Cycles become irregular
You may notice:
Poor sleep
Anxiety or mood swings
Heavier or irregular periods
Brain fog
Feeling “off” without clear reason
Menopause (around age 51)
Menopause is officially reached after 12 straight months without a menstrual period. In the United States, the average age is around 51 to 52. After menopause, ovarian production of estrogen and progesterone drops substantially. That change can affect hot flashes, sleep, vaginal dryness, urinary symptoms, sexual comfort, bone health, and long-term cardiometabolic health.
Estrogen drops significantly
Progesterone is very low
Testosterone also declines
You may notice:
Hot flashes / night sweats
Vaginal dryness
Low libido
Fatigue
Weight gain (especially midsection)
Skin and hair changes
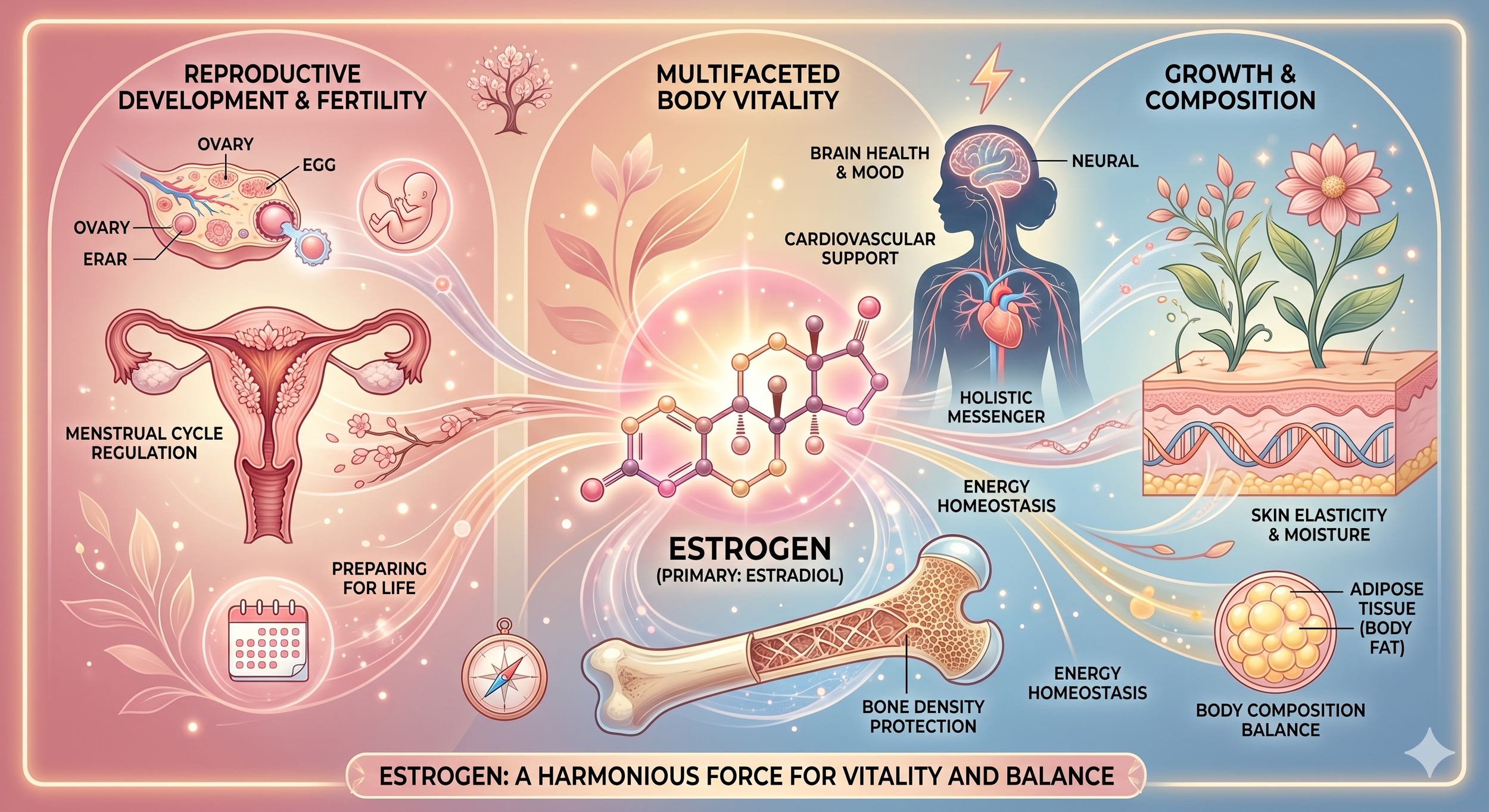
Estrogen: not just a “female hormone”
Estrogens play a major role in puberty, the menstrual cycle, fertility, pregnancy, menopause, bone health, and more. They are also important in men, though at lower levels. Estrogen influences the brain, bones, cardiovascular system, skin, and the vaginal and urinary tissues.
What low estrogen can look like
Low estrogen often shows up as hot flashes, night sweats, vaginal dryness, painful sex, sleep disruption, mood changes, brain fog, joint discomfort, skin dryness, and accelerated bone loss. In early or surgical menopause, low estrogen can also raise longer-term health concerns if symptoms and deficiency are significant.
What high or imbalanced estrogen can look like
This depends on the life stage. In cycling women, relative estrogen excess can be associated with heavy bleeding, breast tenderness, bloating, and PMS-type symptoms. In perimenopause, estrogen can fluctuate wildly, so symptoms may feel inconsistent month to month. Lab interpretation needs context, not just one number.
Why test estrogen
An estrogen test can be helpful when looking at fertility, menstrual changes, ovarian function, menopausal transition, or unexplained symptoms. But one key counseling point is that estradiol levels can swing a lot in perimenopause, so labs should be interpreted with symptoms, age, cycle pattern, and other markers such as FSH and sometimes LH.
Estrogen therapy options
For menopause care, estrogen may be prescribed as pills, patches, gels, sprays, vaginal rings, vaginal creams, or vaginal tablets. Systemic estrogen is the most effective treatment for hot flashes and night sweats, while low-dose vaginal estrogen is often used more specifically for dryness, painful sex, and urinary or vaginal tissue symptoms. Women with a uterus generally need progesterone or a progestogen added to systemic estrogen to protect the uterine lining.
Common formulation examples
Common estradiol patch strengths include 0.025, 0.0375, 0.05, 0.075, and 0.1 mg/day.
Estradiol vaginal cream 0.01% is one common local option for genitourinary symptoms.
Injectables are often prescribed starting at:
These are examples of available formulations, not a universal recommendation. Dose selection should match symptoms, goals, age, uterus status, and risk profile.
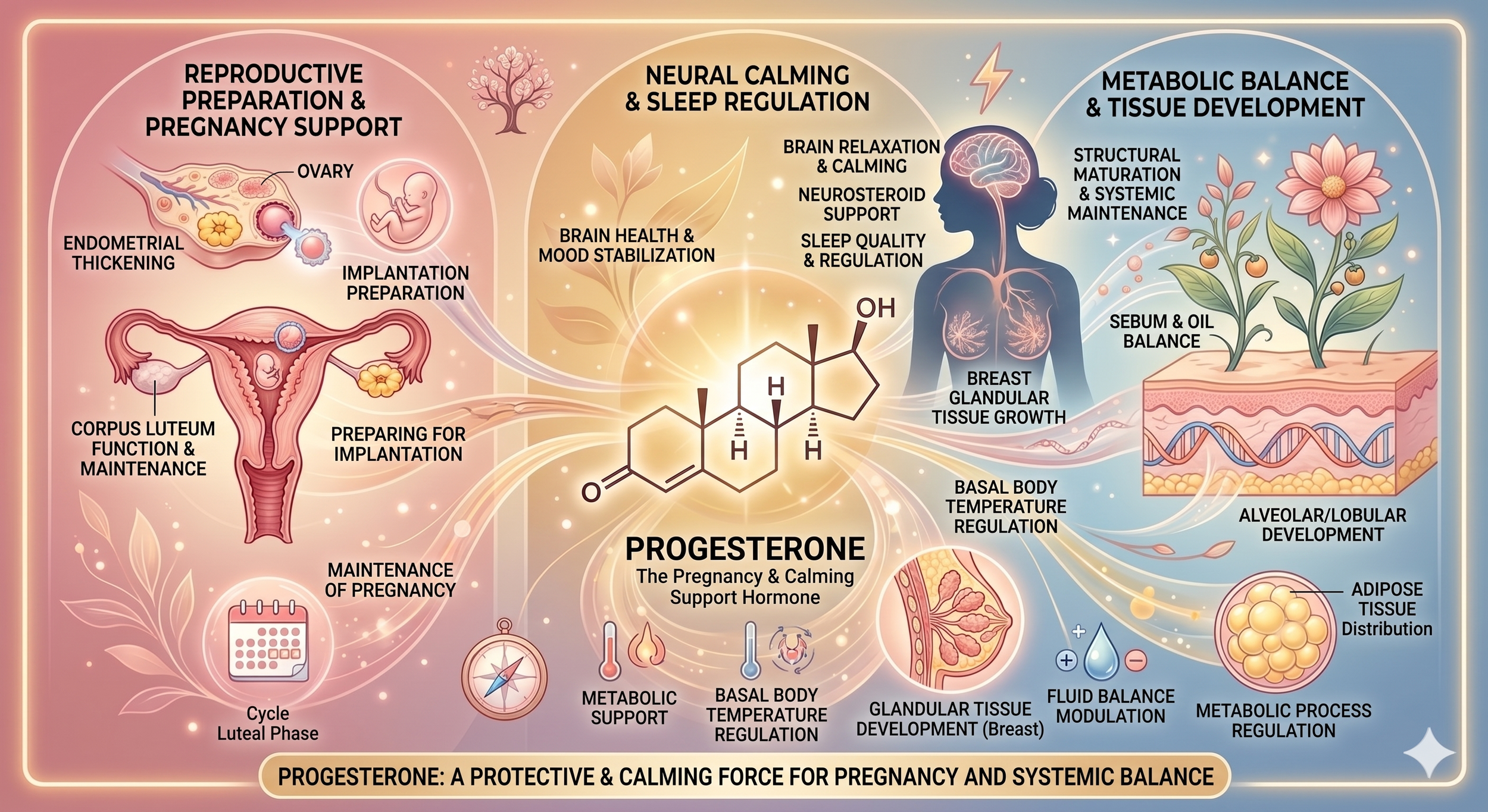
Progesterone: the hormone that often gets overlooked
Progesterone is made mainly by the ovaries and rises after ovulation. It helps prepare the uterus for pregnancy and is central to normal cycle function. In practice, many women feel the effects of low progesterone before they recognize it on paper, especially in perimenopause when ovulation becomes less predictable.
What low progesterone can look like
Low progesterone may show up as irregular cycles, spotting, heavier periods, poor sleep, feeling more anxious before the period, shortened cycles, or infertility when ovulation is inconsistent. In perimenopause, progesterone can decline earlier than estrogen because ovulation gets less reliable.
Why progesterone matters in hormone therapy
Progesterone is not just about the cycle. In a postmenopausal woman with a uterus, progesterone or a progestogen is commonly used with systemic estrogen to reduce the risk of endometrial overgrowth. That is one of the most important reasons clinicians ask whether the uterus is still present before prescribing systemic estrogen.
Progesterone therapy options
Progesterone is commonly used orally. FDA-approved progesterone capsules are available in 100 mg and 200 mg strengths, and labeled menopausal dosing examples include 200 mg at bedtime for 12 days of a 28-day cycle in certain postmenopausal regimens using estrogen. Some products and clinicians also use other progestogens depending on the goal and formulation.
Progesterone is often part of the safety plan when we use estrogen in someone who still has a uterus, and it can also be a meaningful hormone in sleep, cycle rhythm, and how someone feels through the month.
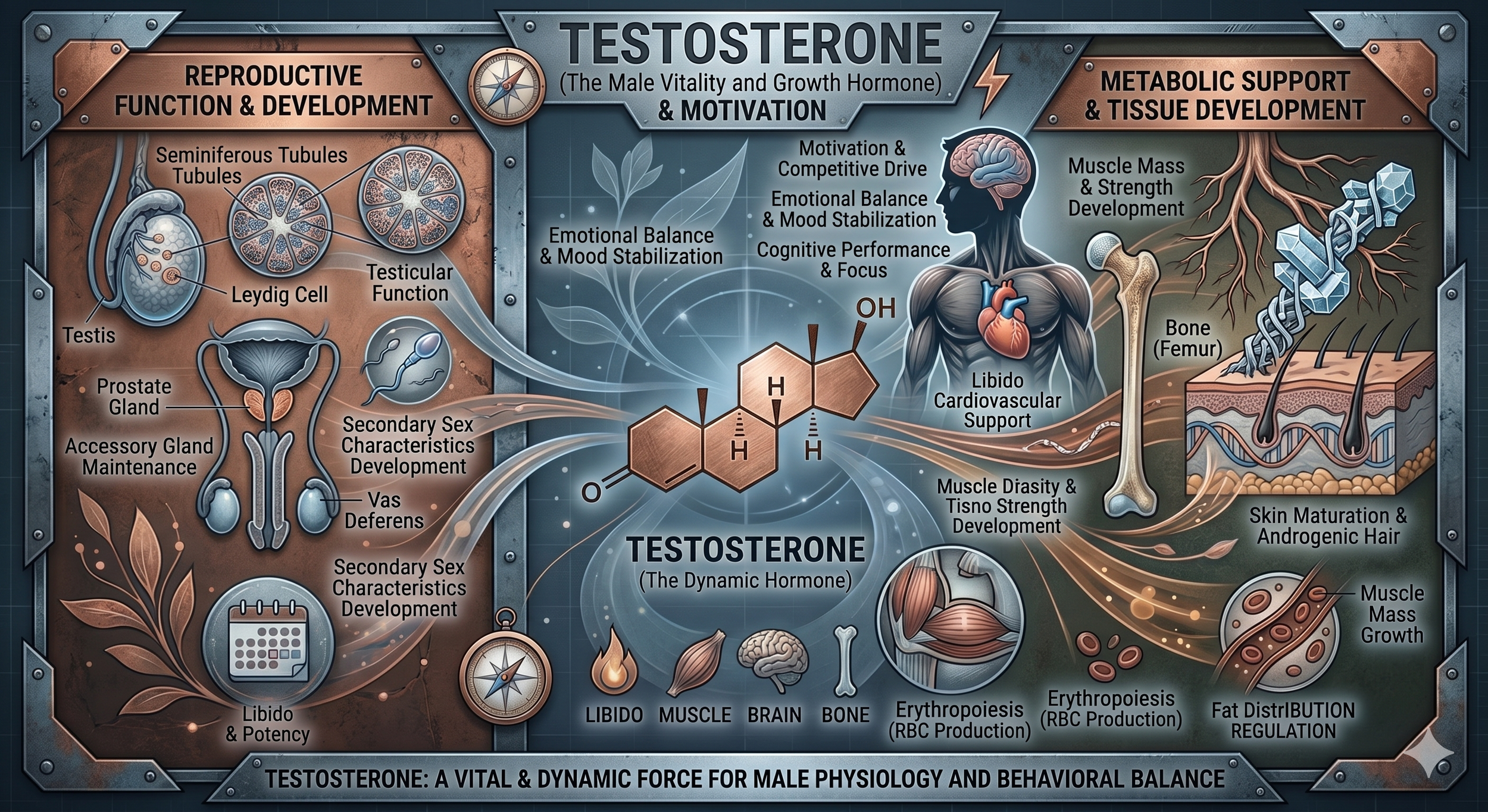
Testosterone: important in women and men
Testosterone is often talked about as a male hormone, but women make and use testosterone too. In both sexes, testosterone contributes to libido, muscle and bone health, energy, body composition, and overall vitality. SHBG also matters because it influences how much testosterone is active and available to tissues.
Testosterone in women
Testosterone can affect desire, arousal, motivation, muscle tone, and body composition in women too. But this is where nuance matters. In the U.S., there is currently no FDA-approved testosterone product specifically for women. The best-supported evidence-based use is for carefully screened postmenopausal women with hypoactive sexual desire disorder, not for every symptom that gets blamed on hormones.
What low testosterone can look like in women
Women may describe low desire, low motivation, poor recovery, decreased strength, lower mood, less resilience, or feeling flat. But these symptoms are not specific to testosterone. Thyroid dysfunction, low iron, sleep loss, stress, depression, medications, and relationship factors can all be part of the picture. That is why libido conversations should be broader than one lab.
Low testosterone in men
Male hypogonadism should be diagnosed only when symptoms are present and testosterone is unequivocally and consistently low on testing. Common symptoms include low libido, erectile issues, fatigue, reduced lean mass, depressed mood, concentration or memory issues, increased body fat, and lower endurance. Guidelines do not recommend routine screening of all men without symptoms.
MEN: GRADUAL TESTOSTERONE DECLINE
Starting in the 30s, testosterone begins to decline.
This is often accelerated by:
Stress
Poor sleep
Alcohol
Metabolic dysfunction
You may notice:
Lower energy
Reduced strength
Increased body fat
Low libido
Brain fog
Decreased motivation
Testosterone therapy options
In men, testosterone therapy may be prescribed as gels and other formulations depending on the case. One FDA-labeled testosterone gel example starts at 50 mg once daily, with labs used for adjustment. In women, testosterone use is typically off-label in the U.S. and should be conservative, goal-specific, and monitored closely for side effects like acne, hirsutism, or voice changes. Formulations include injectables, oral and creams.
The other hormones that matter
FSH and LH
FSH and LH are signaling hormones from the brain that help regulate ovarian function. In menopause, FSH tends to rise while estradiol falls. But in perimenopause, those numbers can fluctuate, so they are helpful pieces of the puzzle rather than a perfect yes-or-no answer on their own.
Thyroid hormones
Thyroid issues can mimic menopause. Low thyroid can look like weight gain, fatigue, mood changes, forgetfulness, and irregular cycles. High thyroid can look like sweating, palpitations, anxiety, and insomnia. This is one reason TSH and sometimes broader thyroid markers matter in a hormone workup.
Insulin
Insulin is central to blood sugar regulation, fat storage, and metabolic health. Insulin resistance can drive weight gain, especially around the middle, along with energy crashes, inflammation, and downstream hormone disruption. When clients say, “I’m doing everything right and still gaining weight,” insulin is often part of the conversation.
Cortisol
Cortisol helps regulate the stress response and affects nearly every organ system. High stress load, poor sleep, inflammation, and overtraining can push cortisol patterns in unhelpful directions, which can worsen sleep, mood, cravings, and recovery.
DHEA-S
DHEA-S is made mostly by the adrenal glands and can convert downstream into other sex hormones. It can be useful when evaluating adrenal contribution, androgen symptoms in women such as acne, hirsutism, or scalp hair loss, and certain ovarian or adrenal disorders.
Symptoms clients often ask about
Libido
Libido is never just one hormone. Estrogen affects comfort, lubrication, and vaginal tissue. Testosterone may affect desire in some women and men. Progesterone can affect sleep and mood. Thyroid, relationship health, stress, antidepressants, blood sugar instability, and body image also matter. A good clinician looks wider than one number.
Hair changes
Hair thinning can be related to menopause, thyroid dysfunction, iron issues, inflammation, high androgen states, nutrient issues, or stress. DHEA-S, testosterone, thyroid markers, ferritin, and the overall metabolic picture may all matter depending on the pattern.
Skin changes
Lower estrogen can contribute to dryness and thinner skin, while androgen imbalance can contribute to acne or oiliness in some people. Skin is often one of the first tissues clients notice changing during perimenopause and menopause because hormone shifts affect collagen, hydration, and tissue quality.
Weight gain and body composition
This is where hormones meet lifestyle. Falling estrogen, lower testosterone, insulin resistance, poor sleep, and chronic stress can all nudge the body toward more abdominal fat, less lean mass, and slower recovery. Hormones matter, but so do protein intake, resistance training, sleep quality, alcohol, and blood sugar control.
WHY LAB TESTING MATTERS
Hormone testing matters because symptoms alone do not tell the whole story. A woman may think she needs estrogen when the bigger issue is thyroid. A man may think he has low testosterone when sleep apnea, obesity, alcohol, or medication side effects are major drivers. A woman with low libido may need support for vaginal estrogen, relationship stress, sleep, and insulin resistance more than she needs testosterone.
A practical hormone lab review often includes some mix of estradiol, progesterone, total testosterone, free testosterone when appropriate, SHBG, FSH, LH, DHEA-S, thyroid markers, and metabolic markers such as fasting glucose, fasting insulin, A1c, lipids, liver health, and inflammation markers, depending on the person and goal. Some people also benefit from more advanced hormone testing depending on symptoms and the clinician’s approach.
You cannot accurately assess hormones based on symptoms alone.
Lab testing helps:
Confirm deficiencies
Identify imbalances
Personalize your plan
Track progress over time
COMMON LABS WE REVIEW
Sex hormones
Estradiol
Progesterone
Total Testosterone
Free Testosterone
SHBG - SHBG binds testosterone and estrogen and affects how much hormone is active. This helps explain why some clients have “normal total testosterone” on paper but still look clinically low or clinically high depending on free hormone availability and the bigger picture.
DHEA-S
Supporting hormones
Thyroid (TSH, T3, T4)
Cortisol (when indicated)
Metabolic markers
Glucose
Insulin
A1c
Lipids
HORMONE REPLACEMENT THERAPY (HRT)
The goal is not to “push hormones high.”
The goal is to restore: physiologic, functional levels
ESTROGEN (WOMEN)
Supports:
Sleep
Brain function
Skin and vaginal health
Bone density
Options:
Injectable
Patch
Cream or gel
Vaginal therapies
👉 If you have a uterus, progesterone is typically required for safety.
PROGESTERONE (WOMEN)
Supports:
Sleep
Calm nervous system
Cycle regulation
Uterine protection
Most common:
Oral capsule
TESTOSTERONE
Women (low-dose)
Improves libido
Supports muscle tone
Enhances motivation and energy
Men
Improves strength, energy, body composition, and libido
Options:
Injectable (most consistent)
Cream or gel
WHY WE OFTEN USE INJECTABLES
Injectables provide:
More consistent absorption
Precise dosing
Easier adjustments
Fewer hormonal fluctuations
WHAT OPTIMIZATION ACTUALLY LOOKS LIKE
Hormones are one piece of the picture.
We also address:
Sleep quality
Strength training
Protein intake
Stress regulation
Alcohol reduction
Blood sugar balance
WHAT TO EXPECT
Gradual improvements over weeks
Personalized dosing adjustments
Ongoing lab monitoring
A plan tailored to your body
We want to understand which hormones are low, high, fluctuating, or being affected by stress, metabolism, thyroid, or age-related change. Then we support the body with the right combination of lifestyle work, nutrient support, and when appropriate, hormone therapy.
What optimization can include
Hormone optimization is not automatically hormone replacement. It may include improving sleep, reducing alcohol, increasing protein, building muscle, managing insulin resistance, reducing excessive training stress, treating thyroid disease, addressing vaginal tissue changes, or using menopause hormone therapy where appropriate. The best plan depends on symptoms, age, uterus status, pregnancy goals, cancer history, clotting risk, and lab findings.
Therapy options: the big overview
For menopause-related estrogen loss, therapy may include oral estrogen, transdermal patches, gels, sprays, vaginal creams, vaginal tablets, or vaginal rings. Women with a uterus usually need progesterone or a progestogen added when systemic estrogen is used. Local vaginal estrogen is typically used for vaginal or urinary tissue symptoms and has much lower systemic exposure than body-wide therapy.
For progesterone support, oral micronized progesterone is a common route in menopause care. For testosterone, men have FDA-approved options, while women in the U.S. do not have an FDA-approved testosterone product and require more careful off-label decision-making.
A few dosing examples clients may hear about
These are examples of formulations people may encounter, not a substitute for individualized prescribing:
Estradiol patch products commonly come in strengths such as 0.025 to 0.1 mg/day.
Oral progesterone commonly comes in 100 mg and 200 mg capsules.
Estradiol vaginal cream 0.01% is one common local product used for vaginal atrophy symptoms.
One testosterone gel product for men has an FDA-labeled starting dose of 50 mg daily.
The important point is that the best dose is not the highest dose. The right dose is the one that improves symptoms, fits the labs, respects safety, and is monitored over time.
What about pregnancy and fertility?
Hormones matter deeply for ovulation, cycle regularity, egg release, implantation, and early pregnancy support. Estrogen and progesterone are central here, but thyroid, prolactin, insulin, and androgen balance also matter. A progesterone test is commonly used to help assess ovulation or support fertility-related evaluation in the right context.
WHY HORMONES FEEL WORSE TODAY
It’s not just aging.
Hormones are impacted by:
Environmental toxins and pesticides
Processed foods
Chronic stress
Poor sleep
Alcohol
Lack of strength training
Have hormone levels really changed over time?
There is real concern about endocrine-disrupting chemicals and environmental exposures. The National Institute of Environmental Health Sciences notes that people can be exposed to endocrine disruptors through food, beverages, pesticides, cosmetics, air, skin, and water. These chemicals can mimic, block, or interfere with hormone action. That does not mean every hormone symptom is caused by pesticides, but it is fair to say our hormonal environment is shaped by more than aging alone.
THE TAKEAWAY
Hormones don’t just affect how you feel.
They affect how you age.
When we understand and optimize them correctly, we’re not just treating symptoms—we’re improving energy, resilience, and long-term health.
Hormones are not just about reproduction. They affect energy, mood, sleep, skin, hair, muscle, weight, libido, bones, and long-term health. Estrogen, progesterone, and testosterone matter in both women and men. Perimenopause and menopause bring these issues into sharper focus, but thyroid, insulin, cortisol, and DHEA-S often belong in the same conversation.
The goal is not to chase one perfect number. It is to understand you, connect symptoms with physiology, use labs wisely, and choose the least aggressive intervention that actually helps. Sometimes that is lifestyle work. Sometimes it is hormone therapy. Often it is both.
Resources
Clue, “Androgens 101.”
Cleveland Clinic, “Hormones: What They Are, Function & Types.”
Office on Women’s Health, menopause overview and symptoms.
ACOG, “Hormone Therapy for Menopause.”
Endocrine Society, testosterone therapy guideline for men.
Global Consensus Position Statement on testosterone therapy for women.
ISSWSH guideline on systemic testosterone for HSDD in women.
NIEHS, endocrine disruptors.
MedlinePlus tests for estrogen, progesterone, SHBG, and DHEA-S.